What is Dandy-Walker Syndrome?
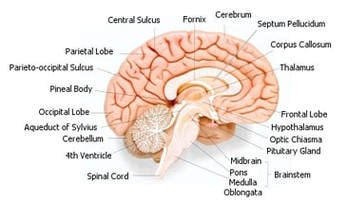
Dandy-Walker syndrome is a condition that affects brain development, primarily development of the part of the brain that coordinates movement (the cerebellum). The central part of the cerebellum, known as the vermis, is absent or very small. Cysts form in the fourth ventricle, which is a fluid-filled cavity between the brainstem and the cerebellum, causing the ventricle to enlarge. The part of the skull that contains the cerebellum and the brainstem, called the posterior fossa, is abnormally large. These abnormalities often result in problems with movement, coordination, intellect, and other neurological functions.
In 80 to 90 percent of individuals with Dandy-Walker syndrome, signs and symptoms caused by abnormal brain development appear within the first year of life. Most children have a buildup of fluid in the brain (hydrocephalus) that causes increased head size (macrocephaly). Affected individuals typically have intellectual disability that ranges from mild to severe, although some have a normal intellect. Children with Dandy-Walker syndrome often have delayed development, particularly a delay in motor skills such as crawling, walking, and coordinating movements. People with Dandy-Walker syndrome frequently experience muscle stiffness and paralysis of the lower limbs (spastic paraplegia), and they may also have seizures. Hearing and vision problems are sometimes a feature of this condition.
Less commonly, other brain malformations have been reported in people with Dandy-Walker syndrome. These malformations include a failure of the brain to divide properly into the right and left hemispheres (holoprosencephaly), underdeveloped or absent tissue connecting the left and right halves of the brain (agenesis of the corpus callosum), a sac-like protrusion of the brain through an opening at the back of the skull (occipital encephalocele), abnormal slits or clefts in the brain (schizencephaly), or a type of birth defect that occurs when the protective covering around the brain or spinal cord fails to close during development (neural tube defect). These additional brain malformations are associated with more severe signs and symptoms.
Dandy-Walker syndrome is estimated to affect 1 in 25,000 to 30,000 newborns. It is estimated that 20 percent of individuals with Dandy-Walker syndrome survive past the first year of life. The most common causes of death in people with Dandy-Walker syndrome are problems related to hydrocephalus or complications of treatment.
Source: http://ghr.nlm.nih.gov/condition/dandy-walker-syndrome
Dandy-Walker syndrome is a condition that affects brain development, primarily development of the part of the brain that coordinates movement (the cerebellum). The central part of the cerebellum, known as the vermis, is absent or very small. Cysts form in the fourth ventricle, which is a fluid-filled cavity between the brainstem and the cerebellum, causing the ventricle to enlarge. The part of the skull that contains the cerebellum and the brainstem, called the posterior fossa, is abnormally large. These abnormalities often result in problems with movement, coordination, intellect, and other neurological functions.
In 80 to 90 percent of individuals with Dandy-Walker syndrome, signs and symptoms caused by abnormal brain development appear within the first year of life. Most children have a buildup of fluid in the brain (hydrocephalus) that causes increased head size (macrocephaly). Affected individuals typically have intellectual disability that ranges from mild to severe, although some have a normal intellect. Children with Dandy-Walker syndrome often have delayed development, particularly a delay in motor skills such as crawling, walking, and coordinating movements. People with Dandy-Walker syndrome frequently experience muscle stiffness and paralysis of the lower limbs (spastic paraplegia), and they may also have seizures. Hearing and vision problems are sometimes a feature of this condition.
Less commonly, other brain malformations have been reported in people with Dandy-Walker syndrome. These malformations include a failure of the brain to divide properly into the right and left hemispheres (holoprosencephaly), underdeveloped or absent tissue connecting the left and right halves of the brain (agenesis of the corpus callosum), a sac-like protrusion of the brain through an opening at the back of the skull (occipital encephalocele), abnormal slits or clefts in the brain (schizencephaly), or a type of birth defect that occurs when the protective covering around the brain or spinal cord fails to close during development (neural tube defect). These additional brain malformations are associated with more severe signs and symptoms.
Dandy-Walker syndrome is estimated to affect 1 in 25,000 to 30,000 newborns. It is estimated that 20 percent of individuals with Dandy-Walker syndrome survive past the first year of life. The most common causes of death in people with Dandy-Walker syndrome are problems related to hydrocephalus or complications of treatment.
Source: http://ghr.nlm.nih.gov/condition/dandy-walker-syndrome

How Dandy-Walker Syndrome Affects Bubbe
At first the diagnosis was both scary and abstract. No one could tell us how the brain abnormalities would contrite to Braxton's future. The first and most obvious symptom is Braxton's muscle tone. He had a very strong back arch, he could hold his head up almost immediately after birth, which was his hyper-tone, not strength as we originally thought. He could push up from his stomach early on as well. However this tendency to extend started to affect his ability to nurse and remain in a seated position. He would push back and away constantly. When he was three months old Braxton developed seizures, the second major symptom of his brain abnormalities. As he grew there were more problems with his muscle control and coordination, many of these problems were probably worsened by his seizure medications, which had the side effect of making him sedated and "floppy". Instead of being able to push up, he became a rag doll, and he can no longer hold up his own head or roll over.
Braxton doesn't have hydrocephalus and instead of the typical larger head, Braxton has a tiny head, microcephaly. This means that everything associated with his head is tiny, his eyes, his throat, his airway. This has caused some complications when Braxton has been admitted to the hospital and doctors expect him to be a certain size, especially when he has needed breathing and feeding tubes.
Braxton has many vision problems, which may or may not be related to his brain abnormalities, which I have outlined on the vision page (http://fortheloveofbubbe.weebly.com/vision.html). He also has the related abnormalities of agenis of the corpus collosum and simplified folds of the brain. We don't yet know how this might affect Braxton, although there is some thought that it can lead to autistic behaviors.
Most recently Braxton has developed problems with feeding and breathing. Tests show he is aspirating his own secretions. We suction his mouth when he has a build up of saliva to help. He is needing a g-tube to feed to reduce the risk of aspiration. We don't know if this sudden change was caused by a seizure, a reaction to his sedating medications, or is a symptom of his brain abnormalities. He is having sleep apnea, which is caused by his brain not recognizing the need to breath. Currently he has very short spells where his oxygen levels drop, but he recovers quickly, so doctors don't think it is causing harm. However these regressions are cause for concern, we want him to grow and progress, lately his development is slowing instead.
At first the diagnosis was both scary and abstract. No one could tell us how the brain abnormalities would contrite to Braxton's future. The first and most obvious symptom is Braxton's muscle tone. He had a very strong back arch, he could hold his head up almost immediately after birth, which was his hyper-tone, not strength as we originally thought. He could push up from his stomach early on as well. However this tendency to extend started to affect his ability to nurse and remain in a seated position. He would push back and away constantly. When he was three months old Braxton developed seizures, the second major symptom of his brain abnormalities. As he grew there were more problems with his muscle control and coordination, many of these problems were probably worsened by his seizure medications, which had the side effect of making him sedated and "floppy". Instead of being able to push up, he became a rag doll, and he can no longer hold up his own head or roll over.
Braxton doesn't have hydrocephalus and instead of the typical larger head, Braxton has a tiny head, microcephaly. This means that everything associated with his head is tiny, his eyes, his throat, his airway. This has caused some complications when Braxton has been admitted to the hospital and doctors expect him to be a certain size, especially when he has needed breathing and feeding tubes.
Braxton has many vision problems, which may or may not be related to his brain abnormalities, which I have outlined on the vision page (http://fortheloveofbubbe.weebly.com/vision.html). He also has the related abnormalities of agenis of the corpus collosum and simplified folds of the brain. We don't yet know how this might affect Braxton, although there is some thought that it can lead to autistic behaviors.
Most recently Braxton has developed problems with feeding and breathing. Tests show he is aspirating his own secretions. We suction his mouth when he has a build up of saliva to help. He is needing a g-tube to feed to reduce the risk of aspiration. We don't know if this sudden change was caused by a seizure, a reaction to his sedating medications, or is a symptom of his brain abnormalities. He is having sleep apnea, which is caused by his brain not recognizing the need to breath. Currently he has very short spells where his oxygen levels drop, but he recovers quickly, so doctors don't think it is causing harm. However these regressions are cause for concern, we want him to grow and progress, lately his development is slowing instead.
More Info....
http://www.dandy-walker.org/
http://ghr.nlm.nih.gov/condition/dandy-walker-syndrome
http://emedicine.medscape.com/article/408059-overview
http://www.dandy-walker.org/
http://ghr.nlm.nih.gov/condition/dandy-walker-syndrome
http://emedicine.medscape.com/article/408059-overview
 RSS Feed
RSS Feed
